Gallstone disease is one of the most expensive digestive disorders, leading to about 1 million gallbladder removal surgeries (cholecystectomies) annually in the United States. Though surgery may relieve acute pain, it often fails to address the underlying cause, leaving some individuals with persistent or new digestive issues.
What Are the Symptoms and Early Signs of Gallstones?
- Sudden, intense pain in the upper right abdomen that is sometimes mistaken for a heart attack due to its intensity and location
- Pain that may radiate to the back or right shoulder
- Episodes of pain lasting 30 minutes to several hours (typically less than six hours)
- Pain often occurring after meals, especially a large, fatty meal
- Accompanying nausea and vomiting
What Causes Gallstones?

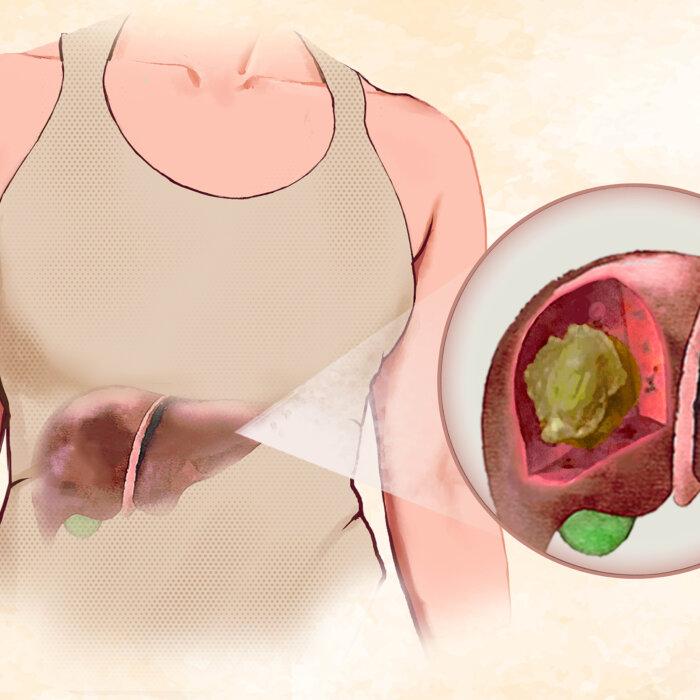
Bile is a fluid produced by the liver, with important roles in digestion, absorption of fat-soluble vitamins (A, D, E, and K), and the elimination of waste products from the body. It contains cholesterol, bile salts, bilirubin, phospholipids, and other substances. From the liver, bile flows into the gallbladder. Here, water and electrolytes are removed to concentrate the bile, making the stored bile more potent.
When dietary fat enters the small intestine, it triggers the release of the hormone CCK. CCK then stimulates the gallbladder to contract, releasing concentrated bile into the cystic duct. The cystic duct joins up with the common bile duct, which enters the small intestine. Then, the bile emulsifies fats, breaking large fat globules into smaller droplets.
If the bile becomes saturated with cholesterol or bilirubin, tiny crystals begin to form. This happens due to excess cholesterol, insufficient bile salts, or both. Bile salts are essential for keeping cholesterol dissolved in bile. Over time, these crystals can grow into gallstones, ranging in size from a grain of sand to a golf ball. There may be one stone or hundreds, and they can either remain in the gallbladder or migrate to the bile ducts.
Recent research has expanded our understanding of gallstone formation beyond the misconception of simply too much cholesterol. Two important elements that contribute to this process are the gut microbiome and the vagus nerve.
The Gut-Brain Connection in Gallstone Formation
The gut microbiome (the community of bacteria in our intestines) and the vagus nerve (a key nerve connecting the brain and gut) play important roles in gallstone formation. Our gut bacteria help modulate bile acid composition and cholesterol secretion, which are crucial for preventing gallstones. The vagus nerve helps the gallbladder contract and release bile properly. It also controls gut motility, which is essential for preventing bacterial overgrowth.When either of these systems is disrupted—for example, by poor diet, antibiotics, or stress—it can lead to changes in bile composition or flow, increasing the risk of gallstone formation.
Additional Factors
Other factors also contribute to the complex process of gallstone formation. These include the following:- Immune system: T-cells and neutrophils increase inflammation and produce substances that help cholesterol crystals stick together.
- Supersaturation of bile: When bile contains more cholesterol than it can dissolve, the excess cholesterol forms crystals. These crystals can clump together over time, eventually developing into gallstones.
- Metabolic factors: Conditions like obesity and insulin resistance alter bile metabolism, leading to higher cholesterol concentrations in bile.
- Dyslipidemia: An imbalance of blood fats, specifically low high-density lipoprotein (HDL) and high triglycerides, increases the likelihood of cholesterol coming out of the bile and forming solid particles.
- Bile stasis: Incomplete emptying of the gallbladder (stasis) concentrates bile and raises stone formation risk.
- Bile acid insufficiency: Bile acids keep cholesterol dissolved. Insufficient bile acid production allows cholesterol to crystallize.
- Hypomotility: Reduced movement (hypomotility) of both the gallbladder and intestines slows bile flow, allowing it to stagnate and become more concentrated, which can increase the risk of crystal formation.
- Hormonal factors: Estrogen increases cholesterol secretion into bile, while both estrogen and progesterone reduce bile salt secretion. Progesterone also slows gallbladder emptying, which can lead to bile stasis.
What Are the Types of Gallstones?
- Cholesterol stones: These account for most stones and contain more than 50 percent cholesterol. They are associated with metabolic disorders such as obesity and Type 2 diabetes and are the most common in Western countries.
- Pigment stones: Pigment stones contain less than 30 percent cholesterol by weight and are either black or brown. Black pigment stones are small and hard, consisting mostly of bilirubin (calcium bilirubinate). They are associated with medical conditions like hemolytic anemia or liver cirrhosis. Brown pigment stones are soft and greasy and represent 5 percent of stones. They are more common in Asia and tend to form in the common bile duct. They are associated with bacterial and parasitic infections, inflammation, and biliary stasis.
- Mixed stones: Sometimes considered a subset of cholesterol stones, these stones contain both cholesterol and calcium bilirubinate.
Who Is at Risk of Developing Gallstones?
Unmodifiable Risk Factors
- Age: Gallstones can occur even in children, but the risk significantly increases with age, becoming four to 10 times more likely after age 40.
- Sex: Women of childbearing age are about twice as likely as men to form gallstones. However, after menopause, the risk starts to equalize.
- Ethnicity: Gallstones are most prevalent among North American Indians, South American aboriginal populations, Mapuche Indians, and Mexican Americans. Sub-Saharan black Africans have the lowest rates.
- Family history: A family history of gallstones increases the risk by nearly five times.
Modifiable Risk Factors
- Diet: Several factors common in the Western diet can elevate the risk. These include high intake of fast food, fructose, saturated fats, and refined carbohydrates and sugar, and low fiber and vitamin C intake. High intake of beans has also been associated with increased risk due to the saponins they contain; thoroughly rinsing cooked or canned beans can help reduce saponins.
- Total parenteral nutrition (TPN): TPN is a method of feeding that bypasses the digestive system, delivering nutrients directly into the bloodstream. Long-term use of TPN significantly increases the risk of gallstone formation, with most patients developing gallbladder sludge within weeks.
- Rapid weight loss: Gallstones develop in 30 percent to 71 percent of individuals undergoing rapid weight loss exceeding 3 pounds per week. This includes those on very low-calorie diets (less than 800 calories per day) or after bariatric surgery.
- Fasting: Prolonged fasting and extended overnight fasting can increase the risk of gallstone formation. Overnight fasting periods of 14 hours or more have been associated with an increased risk of hospitalization for gallstone disease. These fasting periods and prolonged fat-restricted diets can lead to gallbladder stasis and sludge formation.
- Obesity: Obesity greatly increases the risk, especially in late teens. There is a 7 percent to 8 percent increased risk per unit of body mass index (BMI), particularly in women. Obesity promotes bile stasis by increasing gallbladder volume when fasting and reducing emptying after eating. Additionally, obesity increases cholesterol production and secretion.
- Metabolic disorders: Components of metabolic syndrome—including abdominal obesity, high blood pressure, high triglycerides, low HDL cholesterol, insulin resistance, and high fasting blood sugar—are all risk factors. Diabetes, which is closely related to metabolic syndrome, also increases the risk.
- Other underlying diseases: Certain diseases, such as cirrhosis, chronic hepatitis C, nonalcoholic fatty liver disease, cystic fibrosis, Crohn’s disease, and sickle cell disease, are linked to a higher risk of gallstones.
- Pharmaceuticals: Certain drugs are linked to an increased risk of gallstone formation or biliary sludge. These include the antibiotic ceftriaxone (especially in children), thiazide diuretics, octreotide (used to treat conditions like acromegaly and certain cancers), H2-receptor antagonists, and proton pump inhibitors (PPIs). PPIs can also disrupt gut microbial diversity, leading to dysbiosis, an imbalance between beneficial and harmful bacteria.
- Lack of physical activity: Sedentary behavior increases the risk of symptomatic gallstones, while regular exercise reduces the risk. Thirty minutes of endurance exercise five times a week was found to prevent 34 percent of gallstone cases in men. Another study found men and women with the highest levels of physical activity had a 70 percent lower risk. Exercise also helps improve metabolic syndrome, further reducing risk.
- Hormones: Pregnant women and women using estrogen replacement therapy or oral contraceptives are at an increased risk due to the hormonal effects on bile and gallbladder function.
- Smoking: Research suggests that smoking may not just increase the risk of gallstones but may cause them.
How Are Gallstones Diagnosed?
First, the examiner will inquire about dietary habits, foods that trigger attacks, and family history.
Next, the examiner will use what is known as Murphy’s sign, pressing on the gallbladder area beneath the right side of the rib cage and asking the patient to take a deep breath. Severe pain that stops breathing is a positive Murphy’s sign that may indicate gallbladder inflammation.
Blood Tests
Blood tests may include a complete blood count (CBC) with differential to assess white blood cells, pancreatic enzymes, and liver function tests, including:- Bilirubin
- Albumin
- Alanine aminotransferase (ALT)
- Aspartate aminotransferase (AST)
- Alkaline phosphatase (ALP)
- Gamma-glutamyl transferase (GGT)
Imaging
Various imaging techniques are used to visualize gallstones and assess their impact on surrounding structures. These include:- Abdominal ultrasound: This is the initial and most common imaging test for gallstones. It is considered the gold standard due to its accuracy, lack of radiation, noninvasiveness, and low cost. Although it is highly accurate for detecting stones in the gallbladder, it is less so for stones in the bile duct.
- Computed tomography (CT) scans: These are not ideal for identifying gallstones but may be used to look for other issues or complications.
- Magnetic resonance cholangiopancreatography (MRCP): An MRCP provides detailed images of the biliary system. It is particularly useful for detecting bile duct stones when ultrasound results are inconclusive or when biliary obstruction is suspected.
- Hepatobiliary iminodiacetic acid (HIDA) scan: Also known as cholescintigraphy or gallbladder radionuclide scan, a radioactive tracer evaluates gallbladder function and bile flow.
- Endoscopic retrograde cholangiopancreatography (ERCP): This is both a diagnostic and therapeutic procedure that allows direct visualization of the biliary system and can be used to remove bile duct stones.
- Oral cholecystography: This rarely used procedure involves the patient ingesting an iodine-based dye, which is concentrated in the gallbladder. X-rays are then taken to visualize the gallbladder and any stones present.
Functional Medicine Testing
In addition to standard diagnostic tests, functional medicine practitioners may order additional tests to identify underlying root causes that may contribute to gallstone formation or other health imbalances. These tests can provide deeper insights into metabolic, hormonal, and nutritional factors affecting the body and help tailor a personalized treatment plan.- Comprehensive hormone panels evaluate hormone levels, including sex and stress hormones, which can influence bile production and gallbladder function.
- Comprehensive stool analyses assess gut health, including microbial composition, digestion, and inflammation, which are all key to overall metabolic and liver health.
- Advanced lipid panels provide a more detailed look at cholesterol and triglyceride levels, offering insight into lipid metabolism beyond what is shown in standard panels.
- Metabolic markers measure various markers related to energy production, insulin sensitivity, and liver function, which are vital for preventing metabolic conditions linked to gallstones.
- Organic acids tests (OATs) analyze urine for markers related to yeast and bacterial overgrowth, vitamin and mineral status, neurotransmitter metabolites, and mitochondrial function. They can reveal gut dysbiosis, oxidative stress, and detoxification issues that may affect liver and gallbladder health.
- SIBO breath tests are ordered when symptoms like bloating, gas, abdominal pain, or altered bowel habits are present.
- Micronutrient testing identifies deficiencies or imbalances in vitamins and minerals that can affect gallbladder health, cholesterol conversion, and overall metabolic function.
- Food sensitivity testing identifies foods that may trigger inflammation or disrupt digestion, potentially affecting bile composition and increasing the risk of gallstone formation.
What Are Possible Complications of Gallstones?
- Acute cholecystitis is inflammation of the gallbladder, typically caused by a gallstone blocking the cystic duct. Symptoms include severe abdominal pain, fever, and nausea. If untreated, it can lead to serious issues like gallbladder perforation (rupture), which is a medical emergency.
- Chronic cholecystitis is long-term inflammation caused by repeated episodes of acute cholecystitis. It leads to thickened gallbladder walls, scarring, and reduced function due to inadequate bile emptying.
- Infection and gangrene: In severe cases of acute cholecystitis, the gallbladder may become infected. Left untreated, this can result in gangrene, where tissue dies due to lack of blood supply.
- Gallstone pancreatitis occurs when a gallstone blocks the pancreatic duct, causing inflammation of the pancreas. This condition can be severe and potentially life-threatening.
- Cholangitis is an infection of the bile ducts due to a gallstone obstructing the common bile duct. It presents with fever, jaundice, and abdominal pain.
- Jaundice: When a gallstone blocks the common bile duct, bilirubin builds up in the blood, leading to yellowing of the skin and eyes.
- Gallbladder cancer: Chronic inflammation from gallstones can lead to abnormal cell changes, potentially resulting in cancer. While most gallbladder polyps are benign, up to 5 percent may be cancerous. Recent studies have also suggested potential links between gallstones and prostate and pancreatic cancers, but further research is needed to confirm the associations.
- Mirizzi syndrome is a rare complication in which a large gallstone gets stuck in the cystic duct or gallbladder neck, compressing the common hepatic duct. This can cause obstructive jaundice, inflammation, and, in severe cases, a fistula between the gallbladder and bile duct.
- Bouveret syndrome is a rare complication in which a large gallstone blocks the stomach’s outlet. It usually affects older people and causes stomach pain, nausea, and vomiting. Doctors may need several tests to diagnose it, and treatment often involves removing the stone through surgery or other procedures.
What Are the Treatments for Gallstones?
- Pain management: Doctors may prescribe pain relievers, ranging from nonsteroidal anti-inflammatory drugs (NSAIDs) to opioids, as needed. Anti-spasmodics may be given to relax smooth muscle and ease discomfort.
- Addressing dehydration: Intravenous fluids may be administered to replace lost fluids and electrolytes.
- Treating infection: Antibiotics may be given if an infection is present.
- Managing nausea and vomiting: Anti-nausea medication may be given, and food and water may be restricted. In severe cases, a nasogastric tube may be used for stomach decompression.
Cholecystectomy
About 25 percent of symptomatic gallstone cases result in gallbladder removal (cholecystectomy), the primary treatment in the United States. Most cholecystectomies are performed laparoscopically, though open surgery may be necessary in some cases. While most surgeries treat symptomatic gallstones, some are done preventatively for high-risk individuals, such as those who have had organ transplants or are at increased cancer risk. Cholecystectomy may also be performed during other abdominal procedures.If underlying causes are not addressed, gallstones can still form in the bile ducts. Additionally, changes to the gut microbiome and metabolism may occur.
Other Procedures
- Choledocholithotomy: This surgical procedure involves directly removing gallstones from the bile ducts. After removing the stones, the surgeon may close the bile duct immediately or place a temporary drainage tube, depending on the situation. The gallbladder is often removed during this procedure to prevent future stone formation.
- Percutaneous cholecystostomy: This minimally invasive procedure involves draining the gallbladder through a small tube inserted through the skin. It is often used as an alternative to cholecystectomy for high-risk patients with acute cholecystitis, particularly those who are critically ill or have severe comorbidities.
- Endoscopic retrograde cholangiopancreatography (ERCP): Discussed previously as a diagnostic procedure, ERCP can remove gallstones from the bile duct but not those still in the gallbladder. During the procedure, the doctor may also perform a sphincterotomy (cutting the sphincter of Oddi) to aid in stone removal or improve bile flow.
- Extracorporeal shock wave lithotripsy (ESWL): Using focused sound waves, ESWL breaks gallstones into tiny fragments. It is effective for functional gallbladders with no more than three cholesterol stones smaller than 30 millimeters. It is often combined with bile acid medication.
- Percutaneous cholangioscopy-assisted lithotripsy: This advanced technique combines direct visualization of the gallbladder (cholangioscopy) with stone fragmentation (lithotripsy) to break up larger stones. While showing promise, especially in those who cannot have surgery, its availability and research on it may be limited.
Medications
- Bile acid medications: Chenodiol and ursodiol can dissolve cholesterol gallstones over months or years, depending on the stone size. They are used after lithotripsy and bariatric surgery or for nonsurgical treatment. These medications alter bile acid balance and the gut microbiome, potentially causing side effects like diarrhea and abnormal liver function. Due to their complex effects, close medical monitoring is essential during treatment.
- Rowachol: This is a proprietary blend containing six plant-based compounds (including menthol, pinene, and borneol) in olive oil. Used in Europe since the 1950s to treat cholesterol gallstones, it may help dissolve stones, reduce bile cholesterol, and ease digestive spasms. Rowachol typically requires long-term use and is sometimes combined with bile acid medications for enhanced effectiveness. While it is available over the counter in some countries, consult a health care provider before use, as its regulatory status may vary.
How Does Mindset Affect Gallstones?
What Are the Natural Approaches to Gallstones?
Anti-Inflammatory Diet
No one diet works for everyone. Food sensitivity testing can help determine which foods are inflammatory for an individual. Overall, a gallstone-prevention diet should be a whole-food, anti-inflammatory diet focused on the following:- Increased fiber intake: Consume more fruits, vegetables, and whole grains. Fiber helps bind bile acids and promote their excretion.
- Healthy fats: Replace saturated and trans fats with unsaturated fats from sources like olive oil, fatty fish, raw or dry-roasted nuts, and avocados.
- Nuts: Consuming 5 or more ounces of nuts per week was associated with a 25 percent lower risk of cholecystectomy in women compared to those who rarely or never consumed nuts.
- Hydration: Drink plenty of water to keep bile adequately diluted.
- Coffee: Drinking coffee with caffeine regularly might help prevent painful gallstones. Interestingly, the more coffee you drink, the more it might help, but not all studies agree. It is important to think about personal tolerance and possible side effects.
Anti-Gallstone Spices
Certain spices have been found in animal studies to help prevent and even reduce cholesterol gallstones. These spices work by lowering cholesterol levels in the liver, improving bile composition, and making it harder for gallstones to form. Some of the most promising spices include:- Turmeric (Curcuma longa), which contains the active compound curcumin. It can also be taken as a supplement for a more therapeutic dose.
- Red pepper (Capsicum annuum), which contains capsaicin as the active compound.
- Fenugreek (Trigonella foenum-graecum) seeds.
- Garlic (Allium sativum).
- Onion (Allium cepa).
Traditional Chinese Medicine
Traditional Chinese medicine (TCM) offers an alternative approach to treating gallstones by addressing overall bodily function and balance. Studies suggest that certain Chinese herbal compounds may help dissolve gallstones and prevent their recurrence.Supplements
When considering natural or herbal remedies, it is vital to check for risks or potential interactions, especially if you have existing health conditions or take prescription medications. It is recommended to consult your pharmacist or prescribing practitioner for personalized guidance on safety and suitability.While it is best to get nutrients from food, that is not always possible. Micronutrient testing and a diet analysis can help guide supplementation. A professional can help with choosing the right form and dose.
- Vitamin C: Vitamin C is required to convert cholesterol into bile acids. A 2021 study in Current Medicinal Chemistry showed that the prevalence of gallstones was about half as high in those with regular vitamin C intake. Since vitamin C is water-soluble, it is important to consume it daily.
- Phosphatidylcholine: This is a key component of bile that helps keep cholesterol dissolved and plays a role in preventing gallstone formation. While supplementation is sometimes used for these purposes, future research is needed to establish its effectiveness.
- Taurine: This amino acid helps bile acids combine properly. Animal studies suggest taurine may lower liver cholesterol and boost bile acid production, potentially helping prevent gallstones. While its role in human gallstone prevention has not been established, taurine plays a key part in healthy bile function.
- D-limonene: This is a component of several citrus oils (orange, lemon, mandarin, lime, and grapefruit). Clinical studies have shown effectiveness in reducing and even dissolving gallstones when injected directly. Oral supplementation may support liver health and cholesterol metabolism.
- Cholagogues (bile-stimulating herbs): Herbs like milk thistle, dandelion root, and artichoke may support gallbladder function and bile flow.
- Betaine hydrochloride (HCl): This is a supplement that can help restore normal stomach acid levels. Low stomach acid, or hypochlorhydria, may contribute to poor digestion, food allergies, and reduced absorption of key vitamins and minerals. This condition can also lead to SIBO, increasing the risk of gallstones.
- Ox bile: Ox bile is often combined with digestive enzymes and taken with meals to aid in fat digestion and absorption of fat-soluble vitamins. For individuals without a gallbladder, it helps compensate for bile that would otherwise be released during digestion. For those with a functioning gallbladder, long-term use may affect the body’s natural bile production, so professional guidance is recommended.
- Tauroursodeoxycholic acid (TUDCA): Used in TCM for centuries, TUDCA is a naturally occurring bile acid used for purposes similar to ox bile. It is formed by combining ursodeoxycholic acid with taurine, making it more water-soluble than ox bile.
- Fish oil: Omega-3 fatty acids can help shift the balance of fatty acids away from inflammatory omega-6s and possibly help prevent stones in rapid weight loss situations. In the 2021 Current Medicinal Chemistry study, 1.5 grams of omega-3s per day for six weeks effectively decreased cholesterol saturation and stone formation.
- Probiotics: The right strains, based on a stool analysis, can help restore balance to the microbiome.
How Can I Prevent Gallstones?
- Eat a healthy diet: Opt for foods such as wild-caught fish (omega-3 fatty acids), fiber-rich vegetables and some fruits (especially leafy greens, berries, and apples), whole grains like quinoa and oats, nuts, seeds (like flaxseeds), and extra-virgin olive oil. Avoid fast food and ultra-processed foods, added sugars and refined carbohydrates (e.g., white bread, pastries), and hydrogenated and partially hydrogenated oils (trans fats), and limit other saturated fats (e.g., fatty cuts of red meat, full-fat dairy).
- Maintain a healthy weight: Aim to lose weight gradually if necessary. Ursodeoxycholic acid and omega-3 supplementation may help prevent stones during weight loss.
- Keep blood sugar well controlled.
- Exercise regularly, aiming for 30 minutes, five days per week.
- Eat meals at regular intervals and avoid overeating.
- Balance hormones: Work with a professional to do this.
- Avoid smoking.
- Consider moderate coffee consumption.




