Nicknamed the “suicide disease,” complex regional pain syndrome (CRPS) is a debilitating chronic condition that causes severe dysfunction in sensory, motor, and autonomic (self-regulating) nerve functions. It may cause the atrophy or wasting of the tissues in the affected area of the body or sometimes excessive hair growth. CRPS manifests as persistent pain and inflammation typically following trauma, surgery, or other medical events, such as stroke or heart attack. In 7 percent of cases, CRPS occurs without any preceding injury or surgery.
Approximately 200,000 individuals in the United States are estimated to be affected by CRPS each year. One study discovered that 49.3 percent of CRPS patients contemplated suicide, and the actual suicide attempt rate was 15.1 percent.
What Are the Symptoms and Early Signs of CRPS?
Both types of CRPS share the same symptoms. Despite its potential occurrence in any part of the body, CRPS commonly affects the limbs, hands, or feet. Trauma or injury to the affected limb typically triggers the onset of CRPS.
CRPS symptoms vary among individuals, usually starting four to six weeks following the inciting incident.
The initial and primary symptom of CRPS is intense, burning pain that is disproportionate to the type of injury. This pain worsens over time and may start at the injury site but spread to the entire limb. The pain can also be constant, intermittent, or exacerbated by touching the affected limb.

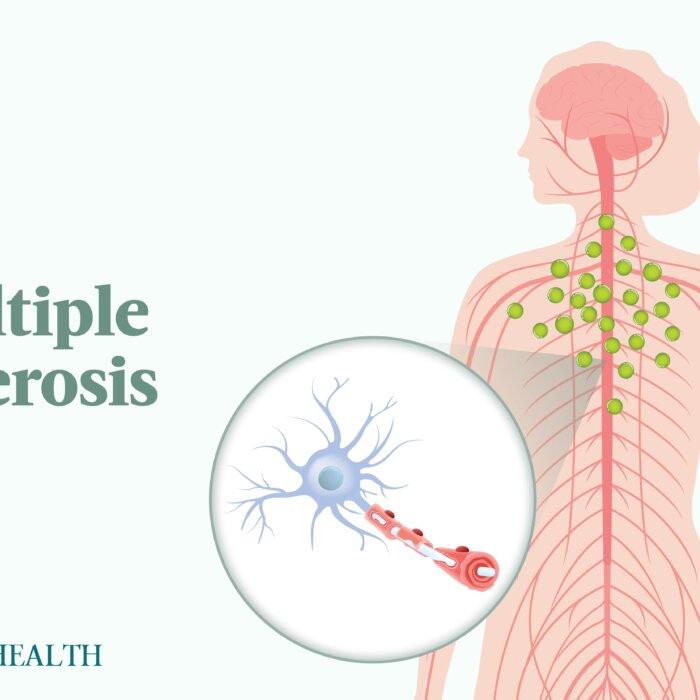
CRPS typically results from an injury or surgery, even if the injury heals or the surgery is successful. The brain activates the sympathetic nervous system, which triggers an inflammation response in the blood vessels, causing swelling and discoloration. The body reacts with an exaggerated pain response, and the brain perpetuates the cycle. Illustration by The Epoch Times
Occasionally, people with CRPS may experience “mirror pain” on the opposite limb, suggesting the involvement of spinal cord neurons. This secondary pain is generally less severe than the primary and tends to diminish as the injured nerves heal.
What Causes CRPS?
While the exact cause of CRPS is unknown, it typically results from trauma or injury or a change in the peripheral or central nervous systems. It can even occur without an injury or because of long periods of immobility. The leading causes are thought to be:
- Fracture: CRPS is often linked with fractures, particularly in extremities. A multicenter study involving almost 600 patients with CRPS revealed that 48.5 percent of the participants had developed their symptoms after a single fracture in specific areas such as the ankle, wrist, scaphoid, or fifth metatarsal. Another study noted type 1 CRPS development within eight weeks after an injurious event. While symptoms improved in some patients after three months, significant overall improvement was not observed after about a year.
- Surgery: CRPS appears to be more commonly associated with extremity surgeries. A retrospective study of 390 patients found that 4.36 percent of those who underwent foot or ankle surgeries developed CRPS. Carpal tunnel surgeries have a 2 percent to 5 percent chance, and Dupuytren contracture surgeries have a 4.5 percent to 40 percent chance of resulting in CRPS. Nerve damage during surgery can result from various factors such as incisions, surgical tools, stitches, and post-surgery scarring. While some cases of nerve damage can be identified and addressed, CRPS may still develop even if the surgery is successful.
- Sprains or strains: Tears in connective tissues, even seemingly minor ones such as ankle sprains, can potentially result in CRPS.
- Burns and cuts: Burns and cuts have the potential to damage underlying nerves, leading to CRPS. Rarely, needle pricks or cuts affecting superficial sensory nerves can cause CRPS.
- Nerve injury: For type 2 CRPS, specific nerve trauma can lead to nerve-associated pain syndrome.
What Are the Types of CRPS?
CRPS is usually categorized into two groups: type 1 (reflex sympathetic dystrophy) and type 2 (causalgia).
- Type 1 (reflex sympathetic dystrophy): Formerly known as reflex sympathetic dystrophy, type 1 CRPS accounts for 90 percent of all cases of CRPS. This type develops following an illness or injury but is not linked to identifiable nerve damage. It is a chronic nerve disorder that commonly manifests in the arms or legs.
- Type 2 (causalgia): Formerly known as causalgia, type 2 CRPS is linked to injury or damage to a particular nerve.
What Are the Stages of CRPS?
In most cases, CRPS progresses through three stages, but not always. Some may experience severe symptoms immediately, while others remain in the initial stage without progressing. The three stages are:
Stage 1
This acute stage of the disease typically lasts one to three months. Symptoms experienced at this stage include:- Skin temperature and color fluctuations: Skin temperature can fluctuate between hot and cold, and skin color and temperature may fluctuate rapidly and inconsistently.
- Intense burning, aching, tingling, or throbbing pain
- Allodynia: Besides the initial pain, individuals with CRPS may experience heightened sensitivity in the affected area, known as allodynia. Allodynia manifests as increased pain in response to light touch or normal physical contact, making using the affected limb particularly painful.
- Hyperalgesia: A person with CRPS might experience intense or prolonged pain following a mildly painful stimulus, such as a pinprick. This phenomenon is referred to as hyperalgesia.
- Skin changes: The affected limb’s skin may become blotchy, purple, pale, red, or mottled, suggesting circulation changes in the region. There may also be increased sweating.
- Edema: Swelling can be significant and localized.
- Accelerated growth of nails and hair
- Muscle spasms and joint pain
- Sleep disorder or insomnia: Sleep disturbances may occur at different stages of the condition.
Stage 2
Also called the dystrophic stage, this stage lasts three to six months. Symptoms include:- Ongoing skin changes: Prolonged insufficient oxygen and nutrient supply to the affected limb in CRPS can lead to changes in skin texture. The skin may look shiny, thin, thick, or scaly. Avoiding contact with painful skin may also contribute to these alterations.
- Cracked and brittle nails
- Escalating pain
- Abnormal hair and nail growth: On the affected limb, CRPS patients may observe rapid, slow, or no growth in hair and nails, as well as patches of excessive or absent sweating. This is because nerves regulate functions and influence blood flow to the area.
- Stiff joints and weakened muscles: To minimize pain, a patient might intentionally limit movement in the affected limb, reducing the flexibility of their tendons and ligaments and weakening their muscles over time.
Stage 3
Also called the atrophic stage, stage 3 manifests after one year. If left untreated, CRPS can progress to a point where moving the affected limb becomes challenging or excessively painful. At this stage, irreversible changes may be observed, including:- Contracture: Tightened muscles and tendons can result in restricted limb movement.
- Muscle atrophy
- Abnormal limb movements: In rare cases of CRPS, individuals may experience abnormal movements in the affected limbs, such as tremors, jerking, or immovable abnormal postures (dystonia). These movements may suggest the possible spread of nerve damage from the original limb to the spinal cord and brain.
- Widespread pain throughout the limb
- Thinning and restructuring of bone: Bone thinning and excess bone growth, potentially impacting the bone marrow, are commonly linked to CRPS.
Who Is More Likely to Develop CRPS?
The following factors may increase one’s risk of developing CRPS following an injury:
- Being in a cast: Prolonged use of casts can restrict limb use and dampen sensory input. Neurons need time to readapt after cast removal.
- Genetics: The role of genetics in CRPS development is not fully understood. However, variants in the human leukocyte antigen and tumor necrosis factor-alpha (TNF-alpha) have been implicated, contributing to an earlier onset and more severe symptoms. Limited retrospective reports suggest the possibility of familial inheritance in some cases.
- Inflammatory changes: Inflammatory changes are considered a key mechanism in the development of CRPS. Increased levels of pro-inflammatory cytokines have been observed in both serum and cerebrospinal fluid of CRPS patients. Neuropeptides released due to tissue injury in CRPS contribute to neurogenic inflammation. However, the redness and swelling in CRPS differ from typical responses to injury.
- Immune system changes: Autoimmune factors are implicated in the development of CRPS. According to one study, intravenous immunoglobulin treatment in CRPS patients has shown significant pain improvement, providing further support for a potential autoimmune aspect in the pathophysiology of CRPS.
- Sex: One study found the female-to-male ratio of CRPS to be 4:1. Another found that females were impacted by CRPS at a rate at least three times higher than males.
- Age: The study that concluded the 4:1 ratio observed a peak incidence of CRPS among females aged 61 to 70. CRPS is rare in children and adolescents, with the earliest onset being at ages 7 to 9 but more often in early adolescence.
- Severe trauma, a lower limb injury, or nerve damage
- Smoking: According to one study, the prevalence of cigarette smoking in individuals with type 1 CRPS was notably higher compared to hospitalized controls (68 percent versus 37 percent).
- Certain medical conditions: These include diabetes, autoimmune disorders, rheumatoid arthritis, fibromyalgia, asthma, osteoporosis, and migraine.
How Is CRPS Diagnosed?
Diagnosing the condition frequently involves relying on clinical observations, as no specific diagnostic tests are currently available. Typically, the diagnosis is made by excluding conditions that exhibit similar symptoms.
The Budapest Criteria
In adults, there are several diagnostic tools for CRPS, including the Veldman criteria, Budapest criteria, and Budapest research criteria, with Budapest Criteria being the most accepted. The Budapest criteria are highly effective and can correctly identify individuals with CRPS 99 percent of the time. However, when it comes to excluding CRPS in those who don’t have it (specificity), they are correct approximately 68 percent of the time.To clinically diagnose CRPS, the Budapest criteria must be met:
- Continued pain: Persistent pain that’s disproportionate to any current inciting event.
- At least one symptom in three of the four categories: sensory (hypersensitivity or pain), vasomotor (temperature, skin color changes), sudomotor (swelling), and motor (reduced range of motion or motor dysfunction).
- At least one sign in two of the following four categories: hyperalgesia (to pinprick), allodynia (to light touch), temperature sensation, deep somatic pressure, or joint movement; temperature asymmetry (more than 1.8 degrees Fahrenheit), skin color changes or skin color asymmetry; edema, sweating changes, or sweating asymmetry; reduced range of motion, motor dysfunction (weakness, tremor, dystonia), or changes in hair, nail, and skin
- No other diagnosis: No other diagnosis better explains the signs and symptoms.
Other Tests
Other tests might be performed to help your doctor confirm the diagnosis, including:- Triple-phase bone scans are the most effective way to exclude type 1 CRPS. In type 1 CRPS, the test reveals increased bone metabolism, with higher substance uptake indicating potentially affected areas.
- Infrared thermography (IRT) is a reliable method for detecting temperature imbalances between limbs, particularly on the affected side of the body. A temperature difference of 0.9 degree Fahrenheit is deemed mild asymmetry, while a difference of 1.8 degrees Fahrenheit is considered significant. IRT can correctly diagnose CRPS in 93 percent of cases, but it is a hard test to obtain.
- Nerve conduction studies (NCS) and electromyography are nerve function tests usually used together to identify nerve damage or other potential causes of your symptoms.
- Diagnostic sympathetic nerve block, or regional anesthesia, determines if your pain is related to the sympathetic nervous system. This involves injecting an anesthetic near your spine’s nerves. If the nerve block alleviates your pain, it helps confirm the diagnosis. Your doctor may also administer a series of blocks for continuous relief. However, despite its utility, nerve block testing for CRPS can yield false-positive and false-negative results because CRPS pain is not exclusively sympathetically maintained, and nerve blocks may also impact nonsympathetic fibers.
- Erythrocyte sedimentation rate (ESR) is a blood test that measures the rate at which red blood cells settle to indicate the presence of inflammation in the body.
- Blood cell count measures the levels of white blood cells, red blood cells, and platelets in the blood and indicates if there is another disease process to consider.
- Serum rheumatologic tests are primarily valuable for confirming clinically suspected diagnoses. Rheumatoid factor testing is suitable when conditions such as rheumatoid arthritis and Sjögren’s syndrome are suspected.
- Ultrasonography might be used to rule out alternative diagnoses leading to one-sided pain, swelling, and variations in skin temperature, such as deep venous thrombosis or impaired arterial blood flow.
- Sweat testing: Sudomotor dysfunction is prevalent in CRPS, and various tests, including subjective indicator-starch powder testing and objective measures, such as resting sweat output, can evaluate sweat output in the affected and unaffected limbs. Sweat testing in CRPS involves assessing abnormal sweating. Q-sweat is a suitable tool for measuring sweat production, with samples taken simultaneously from both sides of the body.
- Quantitative sudomotor axon reflex tests are stimulative examinations that assess sweat output in reaction to a cholinergic challenge transmitted via a weak electrical current through the skin (iontophoresis).
What Are the Complications of CRPS?
The complications of CRPS include:
- Cognitive issues and impaired judgment
- Depression: CRPS can significantly impact an individual’s mental health, leading to conditions such as depression and anxiety.
- Reduced muscle size or strength in the impacted limb
- Extension of the condition to other body regions
- Tissue atrophy of the affected limb: Avoidance or difficulty in moving an arm or leg due to pain or stiffness may lead to deterioration and weakening of the skin, bones, and muscles.
- Involuntary muscle contractions
- Adrenal insufficiency: Adrenal insufficiency arises when the adrenal glands produce insufficient cortisol hormone.
- Gastroparesis: Also called delayed gastric emptying, gastroparesis hinders the movement of food from the stomach to the small intestine without any blockage in the digestive tract.
- Irritable bowel syndrome (IBS): IBS is a prevalent condition marked by abdominal discomfort linked to changes in bowel movements.
- Contracture
What Are the Treatments for CRPS?
While a cure for CRPS doesn’t exist, symptoms may improve or cease spontaneously in most cases. Approximately 85 percent of individuals with CRPS typically undergo a gradual decrease in pain and some of their symptoms during the initial two years.

There is no established and proven treatment approach for CRPS and no extensive randomized controlled studies examining treatments.
CRPS treatment is complex and may not wholly alleviate symptoms, especially if initiated late. Treatment strategies vary based on symptom severity and disability levels, guiding the choice of specific techniques or a combination of approaches. The main objective of all CRPS treatments is to enhance mobility and usage of the affected limb. The different treatment strategies include:
1. Pain Management and Physical Therapy
Pain management in CRPS aims to improve functionality and well-being, thus facilitating rehabilitation. Medications, including those for pain relief and sleep, are commonly used.Physical therapy is the first-line and most crucial treatment for CRPS. Its goals include desensitization, strengthening, increased range of motion, and vocational rehabilitation. Physical therapy includes physiotherapy and occupational therapy. Keeping the affected limb or body part moving is essential for improving blood flow, lessening symptoms, and maintaining flexibility, strength, and function.
Treatment begins with gentle desensitization and may include heat, cold, massage, and contrast baths. As the patient progresses, more aggressive exercises such as range-of-motion exercises, stress loading, isotonic strengthening, and aerobic conditioning are introduced.
2. Drug Therapy
Several classes of medications have demonstrated effectiveness in treating CRPS, especially when administered early in the disease. However, none of these drugs is approved by the U.S. Food and Drug Administration (FDA) specifically for CRPS, and there is no one-size-fits-all guarantee of effectiveness for any single drug or combination. The medications used often include:- Nonsteroidal anti-inflammatory drugs (NSAIDs), including over-the-counter aspirin, ibuprofen, and naproxen, are used to treat moderate pain and inflammation.
- Bisphosphonates, such as high-dose alendronate or intravenous pamidronate, are administered to minimize bone changes.
- Corticosteroids, including prednisolone and methylprednisolone, can address inflammation, swelling, and edema.
- Acetaminophen may alleviate pain associated with bone and joint inflammation.
- Topical analgesics: Pain-relieving ointments, sprays, creams such as lidocaine, and patches such as fentanyl are sometimes recommended to reduce allodynia. Although lidocaine patches can be beneficial for focal CRPS symptoms, they may not be effective for widespread pain.
- Botulinum toxin injections can be beneficial in severe cases, particularly for relaxing contracted muscles and restoring normal hand or foot positions.
- Antidepressant drugs: Certain types of antidepressant drugs are standard treatments for CRPS, even in non-depressed patients. These drugs can offer desirable effects such as pain reduction, improvement in depressive symptoms, and sedation, which is beneficial for those with sleep problems.
- Blood pressure medications: Blood pressure drugs, such as prazosin, can impact the sympathetic nervous system.
- Sleeping medications
3. Psychotherapy and Behavioral Interventions
Severe CRPS can lead to secondary psychological issues such as depression, anxiety, and occasionally post-traumatic stress disorder (PTSD). These conditions may exacerbate pain, limit activity and cognitive function, and hinder individuals from seeking medical care and participating in rehabilitation. High levels of adrenaline-like chemicals linked to depression can make CRPS worse by causing increased sensitivity in the central nervous system. Psychotherapy is thought to work in CRPS by reversing this effect.While limited scientific evidence supports the effectiveness of behavioral interventions in CRPS, they are still recommended as part of a comprehensive treatment plan. Several studies indicate that cognitive behavioral therapy (CBT) can be beneficial in long-term pain management.
4. Intervention Therapy
Nerve blocks, involving injecting a local anesthetic to numb nerves, often provide significant pain relief, facilitating more effective therapy, enhancing mood, and improving overall activity levels. Different types of nerve blocks include:- Sympathetic blocks: Lumbar (lower back) sympathetic nerve blocks are commonly used to treat lower extremity symptoms, while stellate ganglion (neck) sympathetic blocks are utilized for managing upper extremity symptoms. Sympathetic hyperactivity is considered a key underlying mechanism in CRPS.
- Spinal cord stimulation (SCS): SCS involves electrically stimulating the dorsal column of the spinal cord using electrodes placed in the epidural space. These electrodes are typically connected to an implanted pulse generator or, in some cases, an external one.
- Dorsal root ganglion stimulation: Targeting the dorsal root ganglion (DRG) is a newer neuromodulation approach than SCS, offering a more focused application of neurostimulation near the spine. A pooled analysis study confirmed the safety and effectiveness of DRG stimulation.
- Deep brain stimulation: Electric stimulation can be administered close to damaged nerves, beneath the skull, and within the brain’s pain centers, a technique known as deep brain stimulation.
5. Spinal-Fluid Drug Pumps
These implanted devices administer pain-relieving medications directly into the cerebrospinal fluid surrounding nerve roots and the spinal cord. This targeted delivery reduces side effects and enhances the effectiveness of low doses of pain medications. However, implant therapy such as these drug pumps is typically considered a final option when all other pain management approaches have been unsuccessful.6. Other Options
- Mirror therapy: Mirror therapy has shown benefits for CRPS type 1 patients with phantom limb (amputee) pain or stroke. Using a large mirror placed between their legs, patients view the reflection of the unaffected limb while hiding the affected one. By moving the normal limb and observing its reflection, the brain is tricked into perceiving painless movement in the affected or absent limb. Regular exercise for 30 minutes daily over four weeks has resulted in significant pain reduction for many patients.
- Graded motor imagery: Graded motor imagery is a therapeutic approach that includes mental exercises such as visualizing the movement of painful body parts without actual physical movement. It aims to “retrain the brain” by using visualization to navigate situations that may trigger pain.
- Aquatic therapy: Aquatic therapy is a form of exercise performed in water that reduces weight-bearing on the lower extremities. It offers an accessible approach to introducing resistance exercises. Hydrostatic pressure in water gently compresses joints, potentially reducing edema.
- Desensitization: Desensitization for CRPS involves gradual exposure to textures, progressing from soft to more textured. This approach aims to normalize cortical organization in CRPS patients by restoring sensory processing.
- Contrast baths: Contrast baths, which involve mild temperature variations, may be beneficial in the early stages of CRPS to enhance circulation. However, in advanced CRPS, where vasomotor changes are prominent, cold water immersion could worsen symptoms, making it generally not recommended for these patients.
- Transcutaneous electrical nerve stimulator (TENS): A TENS unit, a small battery-operated device, may provide pain relief by blocking nerve impulses.
How Does Mindset Affect CRPS?
Here are several ways a positive mindset may affect CRPS:
- Improved prognosis: The increased psychological distress encountered during the initial physical injury linked to the onset of CRPS could influence the condition’s severity and long-term outlook. A positive mindset can potentially mitigate psychological distress, thus contributing to improved prognosis.
- Better coping: Some doctors believe that a person’s response to a stressful life event, influenced by the person’s mindset, can initiate CRPS, though most disagree. However, a positive mindset can contribute to developing and implementing effective coping strategies. This may involve engaging in activities that distract from pain or adopting a proactive approach to managing CRPS symptoms.
- Reduced pain: The pain intensity from CRPS can increase due to alterations in surroundings or increased emotional stress. In addition, the perception of pain is subjective and can also be influenced by a patient’s mindset. Therefore, a positive mindset could plausibly contribute to reduced emotional stress and pain perception, leading to reduced pain.
- Emotional well-being: CRPS can lead to emotional distress, including anxiety and depression. A positive mindset can act as a protective factor, promoting emotional well-being and resilience in the face of chronic pain and potentially reducing the risk of suicide associated with depression.
What Are the Natural Approaches to CRPS?
There are several natural ways to manage CRPS. In one case, a wheelchair-bound 35-year-old woman with CRPS achieved significant, sustained, and long-term improvements in her symptoms after receiving treatment with conventional medicine and traditional Chinese medicine (TCM), consisting of acupuncture, moxibustion, and herbal medicines. However, the authors of the report noted that, due to combining treatments, it was difficult to “distinguish the effects of individual treatments.” They also could not determine if the success of the treatments was due to their summation or to the “amplification” of the treatments.
Before starting to use any of these, consult your doctor first.
1. Herbal Medicines
Several herbal medicine formulas have been used to treat CRPS, including:- Baekhaoleejung-tang: This herbal decoction was used in the treatment of the above case. Among its ingredients, the root of the Cynanchum wilfordii plant has anti-inflammatory, antioxidant, and antibacterial properties; the dried twigs of the Cinnamomum cassia plant have been traditionally used to treat chronic pain, anxiety, and depression; and Chinese peony root, the dried root of Paeonia lactiflora, is effective in alleviating various types of pain.
- Hyangsayangwi-tang: This is the other herbal decoction used in the above example. Among its ingredients, Ginseng radix’s (ginseng root) main active ingredients, ginsenosides, have analgesic effects; the dried peel of the fruit of Citrus unshiu, commonly known as satsuma mandarin, has been used in traditional Chinese and Japanese medicine for muscle pain relief; and the dried rhizome of ginger exhibits analgesic properties and can modulate pain through diverse mechanisms.
- Yokukansan: Also called Yi Gan San, Yokukansan’s components include Glycyrrhizae radix, Bupleuri radix, Uncariae uncis cum ramulus, and Cnidii rhizome, which all possess pain-relieving properties. Thus, Yokukansan has been used in the treatment of diverse pain conditions, such as fibromyalgia, phantom limb pain, headache, and trigeminal neuralgia. It has also been successfully treating patients with neuropathic pain, including CRPS patients. Yokukansan has even demonstrated greater effectiveness when compared to conventional medications, including tricyclic antidepressants, carbamazepine, gabapentin, and opioids.
- Boiogito: The Boiogito formula consists of six herbal extracts, including Sinomenium stem, Astragalus root, Atractylodes lancea rhizome, jujube, Glycyrrhiza, and ginger. With magnoflorine derived from Sinomenium stem as the primary constituent, the herbal medicine has anti-osteolytic and anti-inflammatory effects. Furthermore, it contains pain-relieving components, such as liquiritin, isoliquiritin, liquiritigenin, and glycyrrhizin. In one case involving a 68-year-old man suffering from CRPS associated with herpes zoster infection, the Boiogito formula effectively helped to relieve his symptoms.
- Keishibukuryogan: Among its ingredients, Paeoniae radix and Cinnamomi cortex possess analgesic and anti-inflammatory properties, and Paeoniae radix can improve blood flow and relieve different kinds of pain. Also called the Guizhi Fuling formula, Keishibukuryogan also played a positive role in treating the 68-year-old man in the above case.
2. Acupuncture
Acupuncture has gained interest as a potential therapy for CRPS. Studies indicate that chronic CRPS patients treated with acupuncture experience reduced pain and depression, improved quality of life, and better motor function. In addition, acupuncture’s positive therapeutic effects may persist over the long term.In one study, two soldiers diagnosed with CRPS after sustaining upper extremity injuries during military operations used conservative treatment to no avail. Scalp acupuncture administered once to twice a week for one to four weeks resulted in an over 80 percent reduction in pain, decreased sensory changes, and improved function. The positive outcomes were sustained at a 20-month follow-up with no recurrence.
Electroacupuncture is a form of acupuncture in which a small electric current is passed between pairs of needles, and it’s becoming increasingly popular. Studies have shown that electroacupuncture relieves mechanical allodynia (pain caused by light touch, like a hand brushing over skin) in rat models of CRPS by inhibiting the activation of an inflammatory protein in certain spinal cord neurons, suggesting it may effectively treat the condition.
3. Bee Venom and Ginseng Pharmacopuncture
Pharmacopuncture is a form of acupuncture that involves injecting herbal medicines, homeopathic substances, or other pharmacologically active compounds into acupuncture points. It combines principles of traditional acupuncture with aspects of pharmacology, aiming to enhance the therapeutic effects of acupuncture.In one case, a 29-year-old man who was diagnosed with CRPS that continued after a toe surgery seven years prior underwent various pain treatments, but his symptoms persisted. He then received bee venom pharmacopuncture, injected weekly at the Xiaxi acupuncture point (GB43) for 14 sessions. Following the treatment, his pain score was reduced from eight to zero. For a four-month follow-up period, he was pain-free, with no new symptoms or adverse events.
The 35-year-old wheelchair-bound woman in the first case study mentioned also received Panax ginseng pharmacopuncture, with herbal medicine derived from ginseng injected at the Xingjian point (LR2) twice weekly. Her foot discoloration and swelling resolved, and additional improvements were reported at a five-month follow-up.
4. Hypnotherapy
One study involving 20 individuals with type 1 CRPS affecting the wrist and hand saw positive outcomes from hypnotherapy, with significant reductions in pain levels, increased range of motion in fingers and wrist, improved pinch and grasp strength, and enhanced overall functionality. All patients reported satisfaction with the treatment, and 80 percent could return to work after an average of 5.4 sessions. Another study involving a teenager with CRPS also demonstrated the effectiveness of hypnotherapy and promoted the safe and cost-effective inclusion of hypnosis in the comprehensive treatment plan.5. Boron Supplementation
Recent attention has focused on the microbiota-gut-brain axis, particularly its involvement in neuroinflammatory disorders such as CRPS. Emerging research indicates potential links between changes in gut microbiota and CRPS development and progression. Individuals with CRPS frequently display dysbiosis, an imbalance in beneficial and harmful gut bacteria, leading to increased gut permeability and systemic inflammation, which contribute to chronic pain. Boron, an essential trace element, shows potential in positively modulating the gut microbiome and exerting anti-inflammatory effects. Studies propose that boron supplementation may alleviate neuropathic pain and improve CRPS symptoms by restoring microbiome balance and reducing inflammation.6. Intravenous Magnesium Sulfate
In one pilot study, eight type 1 CRPS patients received intravenous (IV) magnesium sulfate infusions over four hours for five days. The treatment was well-tolerated and significantly reduced pain compared to the initial assessment. It also enhanced the patients’ sensory function and significantly improved their impairment level and quality of life. However, a later larger study didn’t find significant differences between the magnesium IV treatment and the placebo.How Can I Prevent CRPS?
Currently, there is no known method of prevention. Initiating early treatment is crucial for slowing the progression of the disease. However, there are several ways to reduce the risk of developing CRPS, including:
- Vitamin C intake: Research indicates that individuals who receive 500 milligrams of vitamin C daily for at least 45 days following a limb fracture or surgery may experience a reduced risk of CRPS or even be able to prevent the condition. However, there has been some mixed evidence.
- Early mobilization: Engaging in early mobilization, such as moving the affected limb as much as medically permitted soon after a stroke, may lower the risk of developing CRPS. In the particular case of stroke, mirror therapy and passive physical therapy are helpful.
- Home exercise programs: In one study involving 56 patients with distal radius fracture, a home exercise program with progressive loading exercises, implemented after cast removal, demonstrated safety and effectiveness in preventing type 1 CRPS. While 16 percent of these patients scored positive on subjective diagnostic criteria, none was diagnosed with CRPS, suggesting the potential preventive value of the home exercise program.



